
This is the second in my series of posts looking at the anatomy of the neck. In the last post I covered the cervical vertebrae, in this post we will look at the ligaments, nerves and blood supply.
Ligaments:
Bones are joined by ligaments. Tendons are something else.
Ligaments can be be in bands or sheets, which are flexible but, with one major exception, are not extensible. They all contain nerve endings. that are important in relation to the movement and position of the body and its reflex mechanisms. Some remain taut throughout a range of motion, whilst those like the cruciates in the knee joint vary in their tension and slackness.
Ligaments in the neck stabilise the extreme ranges of motion which are inherent in the structure of the cervical vertebrae. The thoracic and lumbar are so constructed as to allow only rotational movement in the thorax or flexion and extension in the lumbar.
Figure A. shows the general arrangement of special vertebral ligaments
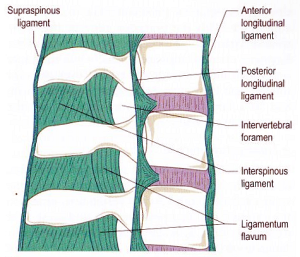
Figure B. Shows the sagittal section of C1 and C2
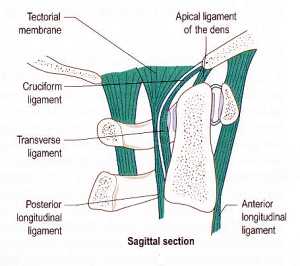
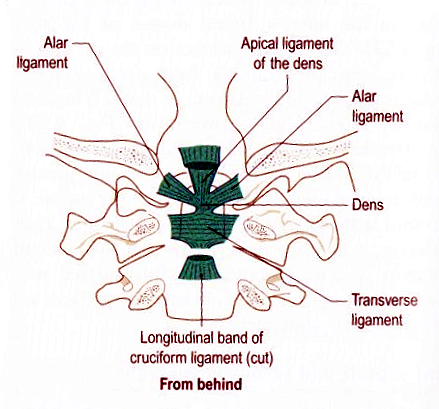
Figure C. Shows the same structure from the rear with C1 and C2 cut from the occiput down.
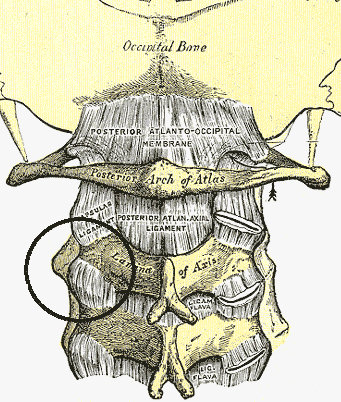
Ligaments, along with muscle tension, hold the head in place. Major ligaments pass across from C1 to the occiput. This joint is the ATLANTO-AXIAL joint.
On the front and back of the whole spine run two long ligamental bands, the anterior and posterior longitudinal ligaments.
The anterior longitudinal ligament has a narrow attachment to the anterior tubercle of the atlas. As it descends to the sacrum it attaches to and crosses the vertebrae and supports the intervertebral discs. It widens as it descends and finally spreads itself over the pelvic (front) surface of the sacrum. Above the atlas it joins into the anterior atlanto-occipital membrane which attaches to the Foramen Magnum. (The Foramen Magnum is the hole in the base skull through which passes the spinal chord)
The posterior longitudinal ligament rises from the 1st sacral ligament, widening as it rises and attaching only to the intervertebral discs. The ligament proper ends at C2, but then it becomes part of the tectorial membrane which itself has connections to C2 at the Dens and other ligaments fixing to the Foramen Magnum.
These two ligaments form a continuous elliptical band, energetically creating deep pathways for us to work with.
The following is a condensation of important membranes and ligaments:-
a) Ligamentum Flavum: On adjacent vertebral bodies from C1 to between L4-L5. The only truly elastic ligament in the body. It assists the post vertebral muscles to maintain an erect posture, and due to its elasticity does not “fold” when returning the torso to upright after flexion.
b) Transverse Ligament of the Axis: From the Dens to the sides of the occiput and then longitudinal fibres go up to the Foramen Magnum.
c) Tectorial Membrane: Arises from the posterior longitudinal ligament and covers the back of the Dens and other ligaments. This rises to the Foramen Magnum where it blends with the Dura Mater (Dura Mater- the hard flexible outer layer of the tube containing cerebro spinal fluid surrounding the spinal column).
d) Apical and Alar ligaments: These create cruciform and medial support from the Dens to the Foramen Magnum.
e) The Ligamentum Nuchae: The nuchal ligament. This attaches to all of the cervical vertebrae from the spine of C7 upwards to the occipital protuberance and crest. It is a rudimentary ligament which in four legged animals is very strong and maintains their head position.
So, if you have got this far you can see that it is essential that these ligaments, from the atlanto-axial joint remain in good condition.
Ligaments thrive on a high fat diet with correct vitamin levels. They degenerate and stiffen with high carbohydrate, sugary diets. Remember fruit has fructose (sugar) in it. Over 25 grams of fructose a day creates a toxic effect in the body (Emmerich, M. (2013)”Keto-Adapted” pub. M and C. Emmerich). So for every 100g of blueberries you may eat, 9 grams are fructose. Add an apple, a potato or some rice and bingo, you are over the limit.
The Blood Supply
I am talking here about the blood supply to the bones and discs of the neck. Blood supply to the muscles will be addressed in the next post focussing on neck muscles.
Imagine the stacked vertebrae, the arterial vessels (vertebral and ascending cervical arteries) run vertically on the bone.

They have branching lateral smaller arteries, passing towards the intervertebral foramen. These create a lattice of vessels over both bone and intervertebral discs.
With age the vessels supplying the discs disappear and it is thought that the mature disc has a blood support from diffusion through the bone. Movement creates pressure changes which speed up diffusion, hence giving truth to the statement that “the slower you move the faster you die”!.
Disc degeneration is a major problem with older, sedentary people, and this lifestyle is being reflected more and more in the population at large. Ageing also “furs up” arteries so that the centre of discs can be much less fluid than the exterior portion, where there is good, if small, arterial contact.
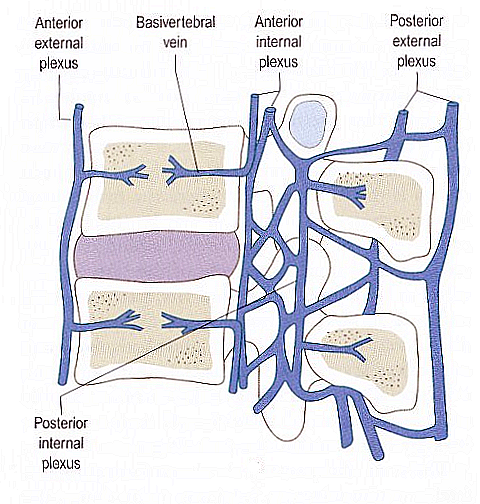
The intervertebral venous system comprises a complex system of plexuses i.e. collecting points, which are drained by intervertebral veins. These eventually connect with the occipital sinuses and movement of the occipto-atlantal ligaments and muscles surrounding them creates a pump-like action sending de-oxygenated and nutrient depleted blood down to the venous systems in the chest and abdomen.
It is almost without doubt that this venous vertebral network plays an important role in the spread of metatastic cancer cells throughout the body. Invariably the secondary metastases of breast and prostate cancer involve this vertebral venous system.
Nerves
Many, many fine nerve filaments and receptors can be found along the ligaments and intervertebral discs, which can explain the pain clients experience when discs have been compressed or over flexed.
The sinu-vertebral nerve connects with the longitudinal posterior ligament (runs from head to perineum) which in turn connects to the venous canals and the spinal chord.
Therefore it is easy to see why pain in the neck and occipital region are so closely associated with ligamental tension. Pain in this area can also be related to nerve tension or “stress” in other areas of the vertebrae anywhere between C7 and L5/S1.
OK, so muscles come next. These are the bits we can touch and via them affect the deeper structures.
I am aware some of this may be complicated but by knowing it you will use this knowledge in your treatments for the benefit of your clients and your growing practice.
Keep at it.