Whole books have been written on this subject. I hope this blog post will stimulate you into working out what you are touching when you treat the neck and the connections with other parts of the body.
Many neck muscles are extremely small and impossible to palpate. Basically, these small muscles are there to balance the head on the vertebral column.
Movement here can be classified as:-
Muscles which move the neck
Muscles which move the head and neck
I am chiefly concerned with those muscles that can be touched, released and toned. Energy projection and structural modification may be required for deep structures. Those marked with an asterisk * are the muscles you can actually palpate.
N.B. For the sake of brevity, I haven’t included pictures for each and every muscle listed. A quick image search on Google should furnish you with those.
Muscles that flex the neck: Longus Colli*, Sternomastoid*, Scalenes anterior*
Muscles that flex the head and neck: Sternomastoid*, Longus Capitis*
Muscles that flex the head ON the neck: Rectus Capitis Anterior
Muscles that laterally flex the neck: Scalenes Anterior, Scalenes Medius, Scalenes Posterior*, Splenius Cervicis
Muscles that laterally flex the head and neck: Sternomastoid*, Splenius Capitis*, Trapezius*,Erector Spinae*
Muscles that laterally flex the head ON the neck: Rectus Capitis Lateralis
Muscles that extend the neck: Levator Scapulae* Splenius Cervicis
Muscles that extend the head and neck: Trapezius*, Splenius capitis*, Erector Spinae*
Muscles that extend the head ON the neck: Rectus Capitis Posterior Major, Rectus Capitis Posterior Minor, Superior Oblique
Muscles that rotate the neck: Semispinalis Cervicis*, Multifidus*
Muscles that rotate the head and the neck: Sternomastoid*, Splenius Capitis
Muscles that rotate the head on the neck: Inferior Oblique, Rectus Capitis Posterior major
(I can hear howls of anguish…..)
You do not have to learn all of these to do an excellent job and in truth you can only touch about ten of them. What follows is a list of the muscles that you are most likely to work with during a normal neck and shoulder treatment. What will make a difference is the ability to relate a movement problem to the major muscles involved. It would be an excellent idea to develop a good working knowledge of the muscles listed below.
Longus Colli: A group of deep muscles originating on the anterior and lateral surfaces of T1, T2, T3 and inserting into C3, C4, C5, C6 and C7. Their main action is to FLEX the neck
Sternomastoid: This originates on the medial third of the clavicle and the superior side of the manubrium and inserts into the mastoid and the occiput. On its own, one muscle rotates the head. e.g. Turns the face from one side to the other. Working together the muscles extend, flex and laterally flex the head.
Scalenes: This ladder like group of muscles originate on the 2nd to the 7th cervical vertebrae and insert into the outer surfaces of the first and second ribs.
outer surfaces of the first and second ribs.
When the scalenes are working on one side of the neck, they rotate the head to the opposite side. Working together they create neck flexion and lateral flexion.
Splenius Capitis: This originates from the lower nuchal ligament and C7 to T4 and inserts into the mastoid process of the temporal bone.
When one side works it creates extension, lateral flexion and rotation of the neck turning the face to the same side. When both muscles work they create extension of the neck.
Longus Capitis: The origin is between C3 and C6 and it inserts into the interior back part of the occiput. One side working creates rotation to the same side. Both sides working creates flexion of he head.
Trapezius: The upper part only originates on the occiput and cervical vertebrae and forms the shape of the neck out to the shoulder point.
There is an anterior portion which inserts into the lateral edge of the clavicle and elevates it, whilst the posterior section elevates and laterally rotates the scapula.
Erector Spinae, sometimes called Sacrospinalis: It is made up of three bi lateral groups of muscles running from the sacrum to the transverse processes of C2 – C7, with attachments to the vertebrae in the lumbar and thoracic regions.
When one side works they create lateral flexion and rotation to the same side.
When working in unison they control flexion of the trunk and neck.
Multifidus: These lie between the spinous and transverse processes of all the vertebrae from S1/L5 to the axis at C2. They have 3 layers which connect each muscle part to the next vertebra above, at the following points:-
From spinous process to spinous process
To the second vertebra above the muscle origin
To the third and sometimes fourth vertebra above the muscle origin
Their job is mainly to stabilise the vertebra and act almost like ligaments in maintaining body position. They assist in rotation when contracting on one side.
Semi Spinalis Cervicis: This is almost an extension of the bulk of erector spinae, having its origins on T7 and T6 and C6 to C4. The fibres insert into the spinous processes of C2 C3 C4 C5.
They create extension of the neck and rotation towards the opposite side.
Levator Scapulae: This muscle starts on the transverse processes of C1 – C4 and inserts into the medial edge of he upper part of the scapula.
If one side contracts it will create lateral flexion of the neck and with both sides working create neck extension.
Other muscles cross the thoracic and neck regions, but these muscles are mainly concerned with facial expression. Opening and closing the mouth and depressing the hyoid bone after it has been lifted by the action of swallowing. One of these muscles is worth palpatory consideration:-
The Platysma: It is a broad sheet of muscle lying in the superficial fascia of the upper chest, starting just below the clavicle. The muscle runs up on top of the sternocleidomastoid to finish in the lower jaw and fascia of the lower face and lip.
It helps to open the mouth but also creates the facial expression of horror by pulling the lower lip down and tightening into the jaw. It can be seen in times of strenuous exertion such as in weightlifting or in runners who are trying to inhale large quantities of air.
It may also stop a collapse of other muscles around blood vessels when this state of strenuous activity exists.
If you want to see more pictures of these muscles you can easily find them online.
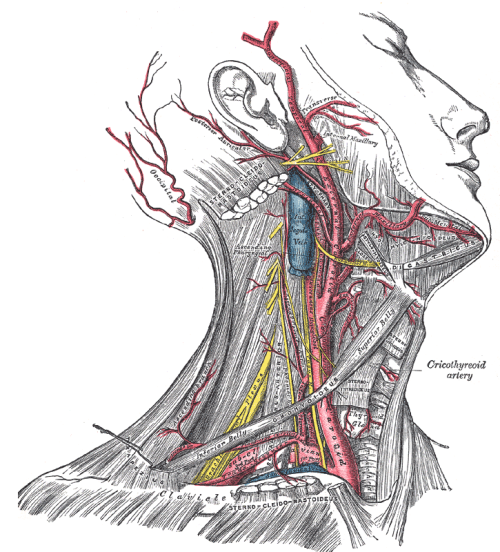
Blood Supply in the Neck
The Arteries
Four major arteries enter the neck from the trunk:-
The left vertebral artery
The right vertebral artery
The left carotid artery
The right carotid artery
These arteries supply blood to the cervical bones and eventually join in the base of the brain forming the basilar artery which supplies blood to the posterior brain. They pass into the skull through the foramen magnum.
The left and the right carotid split in the neck from the carotid artery to form left and right internal and external carotid arteries. The internal ones pass into the skull where they branch beneath the brain and supply blood to the front of it.
The external carotid arteries supply blood to neck muscles, skin and peripheral structures of the head. Three drainage systems return deoxygenated and de-nourished blood to the heart.
Veins
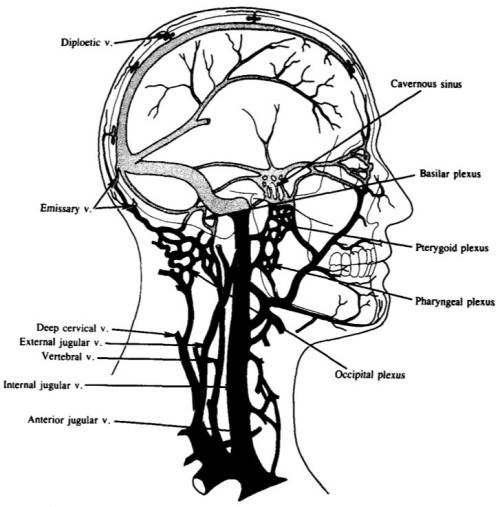
Left and right vertebral veins
Left and right jugular veins
Left and right dural venous sinuses
These vertebral veins descend through the vertebra foramina, draining blood from the spinal chord, cervical vertebrae and neck muscles.
The jugular veins drain the superficial structures of the head and sit outside the vertebral veins.
Dural venous sinuses are large cavities in the upper dura mater which drain the brain and pass this blood into the left and right internal jugular veins which descend back into the neck, to the chest and the heart.
Relationship of structure and blood vessels at C6
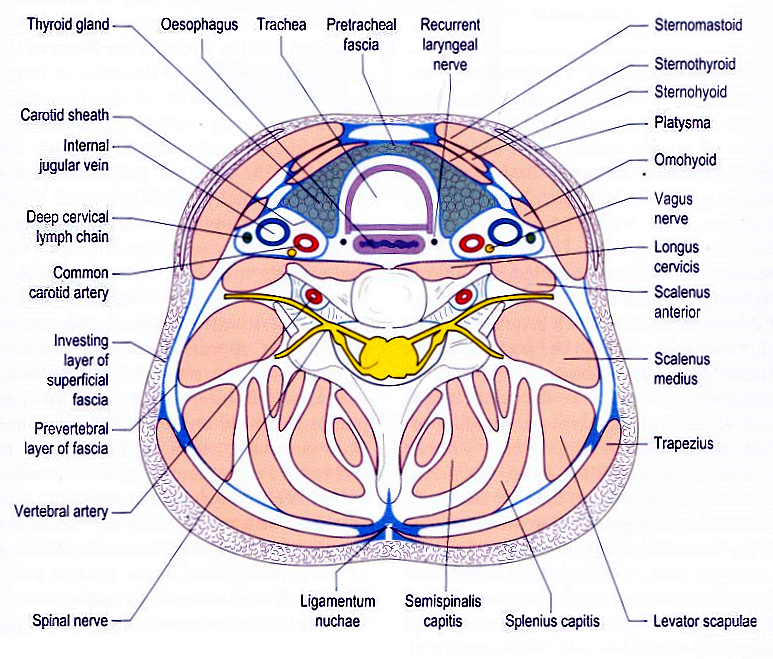
Transverse section of the neck at the level of C6
I thought you should see a cross section at C6. Look for the vertebral arteries supplying blood to the vertebrae, and note how deep are the carotid arteries supplying blood to the brain and the arterial offshoots to muscles and other tissues.
The jugular vein is more available to our touch BUT KNOWING WHERE IT IS allows us to work safely and without interfering with its function.
On a personal note, writing this blog has made me realise how little of the practical “What goes where” anatomy is taught to bodywork students.
To really make a change in the physical, psychological and emotional state it is essential to learn as much of this as you can. Knowing this information has gone a long way to making my practice the success it is. It adds a really powerful dimension to all of my bodywork. The more I know the more I can apply. The pieces of the puzzle come together and I can do marvellous things for my clients all because I KNOW what is under my hands and what the connections are in the rest of the body.
Next up…..Muscles and the meridian positions.